

If you’ve found this page, you either have pelvic organ prolapse or you suspect you do. The good news is, POP happens to the vast majority of women, so you are not alone. The bad news is, there isn’t a lot of research done in this area, so it can often feel like there are no answers to your questions and there is no data set specifically for you.
What’s happening with your POP is unique to you and your situation—everyone’s anatomy is different, so what works for one person or happens to one person may not work for or happen to you. It can be frustrating.
As a disclaimer, I am not a medical professional and nothing written in this site should be taken as medical advice. You should always seek counsel from a Urogyn and a Pelvic Floor PT for diagnosis and treatment.
That being said, over the past year I’ve found some incredible resources that I’d love to share. It took me hours of digging to find this information, and now hopefully, you won’t have to do quite as much digging to get answers.
What is prolapse?
You’ve probably read this description on 100 different websites by now, but POP is when one or more of your pelvic organs descend into the vaginal space. Most common is cystocele, where the bladder descends and pushes the vaginal wall down and sometimes out of the vagina. Rectocele is similar but it happens on the back wall when the rectum bulges into the vagina from the back wall. Thirdly, is uterine prolapse where the cervix descends and can push out of your vagina blocking entry. (Some lowering of the cervix is completely normal after birth, and don’t forget the cervix moves depending on where you are in your cycle). There’s a fourth type: enterocoele which occurs more often in people who have had a hysterectomy and is when the small intestines descend between the rectum and vagina.
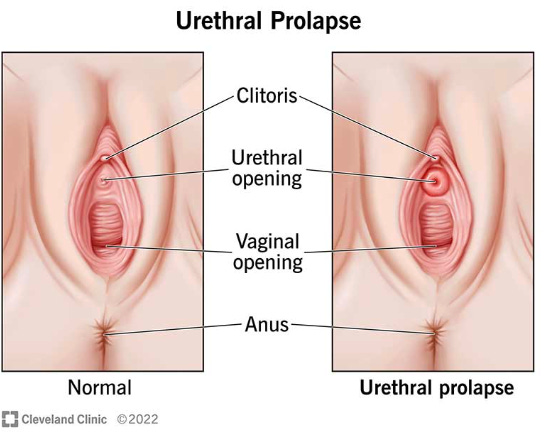
It’s also possible to have anatomical changes to your urethra and the surrounding tissue. This can come in the form of urethrocele where the tissue protrudes from he opening, a hypermobile urethra when a once more stable urethra becomes mobile after birth, urethral swelling for unknown reasons, and the infamous walnut. The Walnut is when the sub-urethral epithelial tissue is exposed or hangs down behind/below the urethra at the vaginal opening. Because this is at the most distal part of the vagina this can cause all the sensations of a prolapse even when no prolapse is present. It can also confuse the results of a POP-Q test as explained by Dr. Fitzgerald in this interview with Dr. Margo Kwiatowski.
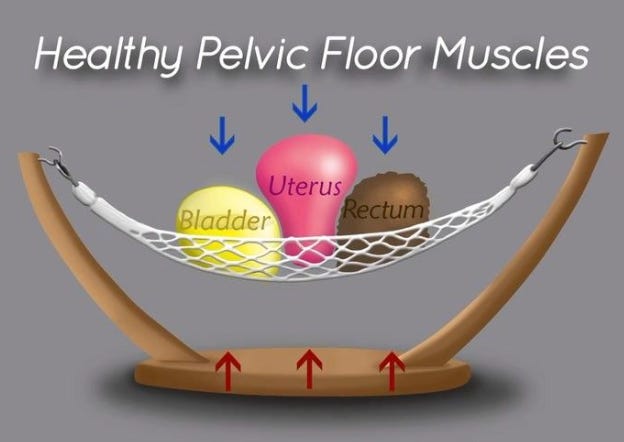
If you’re like me, then you’re wondering, well hold on, if the pelvic floor muscles hold this thing up, can’t I just strengthen them? What exactly is between the bladder and vagina and bladder and rectum? What’s holding these things up if the muscle is just a hammock underneath?
The strength question is extremely complex and will depend on your hormones, degree of injury, tension, and much much more.
This image is the best I’ve seen for showing exactly what else is in there. You have layers of fascia between the organs, and the fascia can become over-stretched, damaged, and weakened. There are tests a PFPT can do to see what’s going on with your fascia that involve a standing pelvic exam while you hold a kegel at 30% strength for a minute.
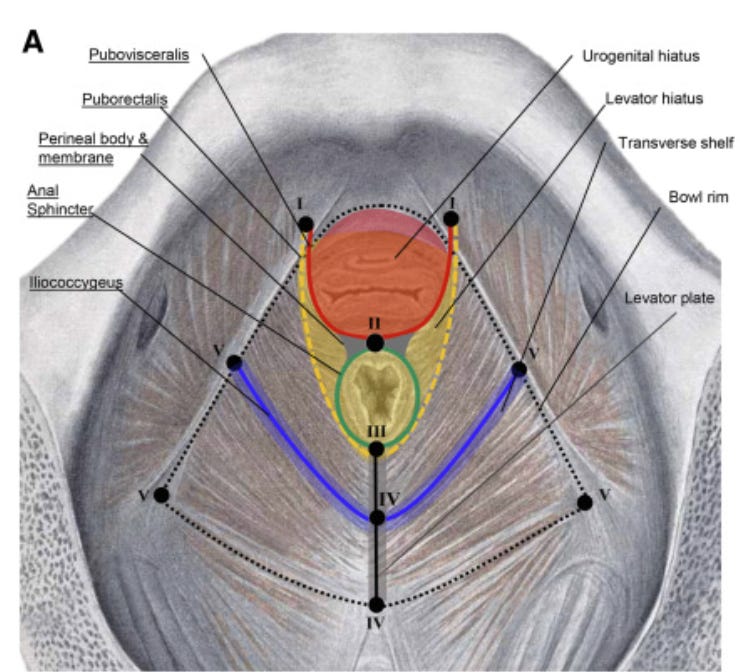
The deepest pelvic floor muscle, the levator ani actually has spaces in it that these organs thread through—thats where the tubes go: the urethra, vaginal canal, and anal canal. That’s why the hammock image isn’t that accurate. The levator hiatus is the name for the opening that the bladder descends through with a cystocele. When your doctor has you bear down while doing an assessment they are often checking this area to see how much descension there is and if there is any ballooning or movement. If you’ve ever heard anyone talking about GH and GH+PB, this space is what they are trying to evaluate in order to determine risk factor for worsening or future prolapse. GH stands for genital hiatus, and is a measurement taken on the outside that is supposed to represent a distance on the inside.


GH is the distance from the middle of the external urethral meatus to the posterior midline of the hymen. PB is the distance from the back wall of th eopening of the vaginal canal to the middle of the anal opening (perineal body). Typically providers want to see GH+PB be less than 7 centimeters.
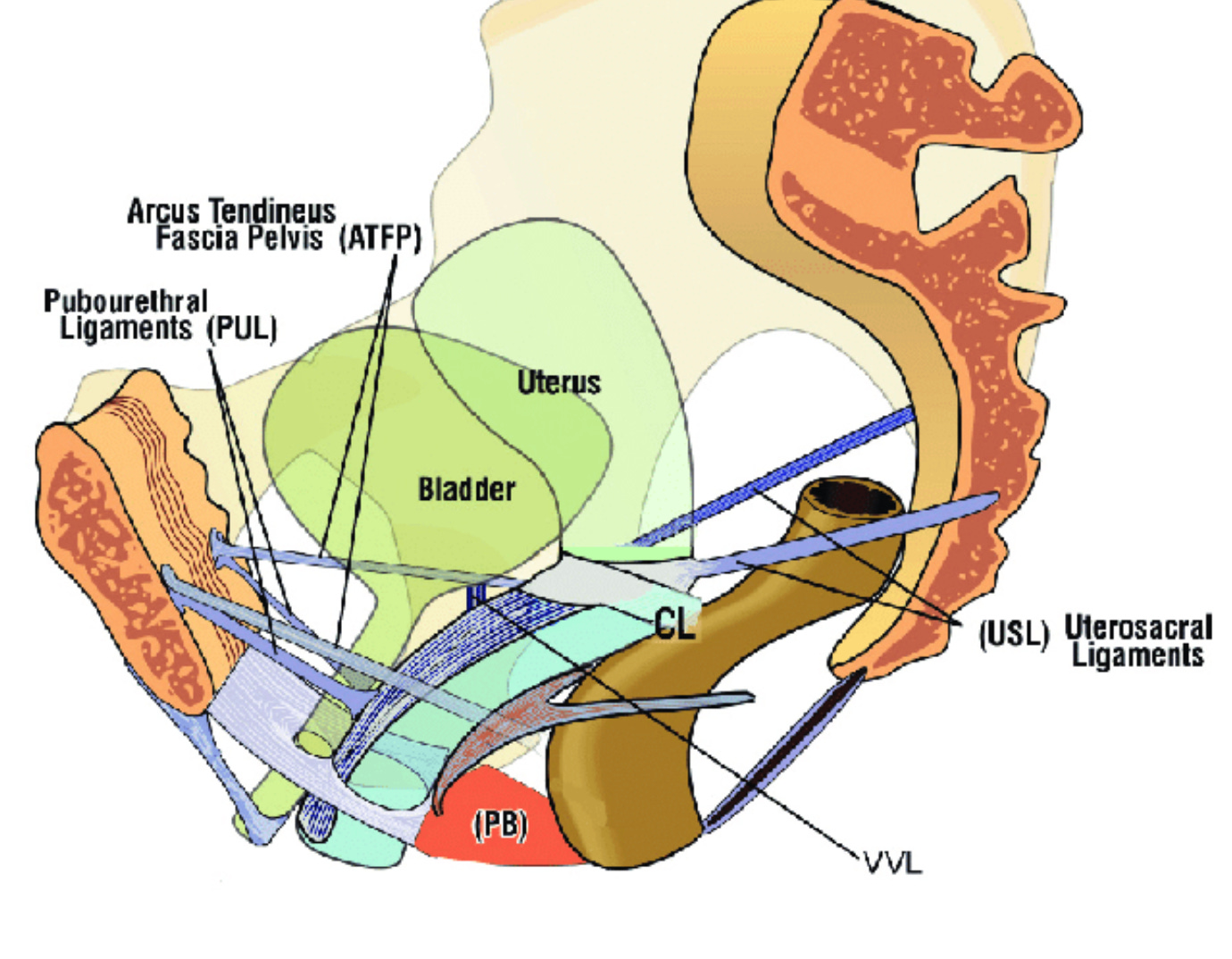
Lastly, you have ligaments holding up your organs. The problem is if you’ve carried a baby, then these ligaments have stretched out. And while these ligaments often shorten and rebound well after childbirth, they can still remain a little slack especially if your estrogen levels are low because you’re lactating. This is one of the reasons PFPTs encourage training like an athlete (depending on your specific situation). Because if you strengthen your accessory muscles (glutes, abdominals, adductors) your organs will be held tighter and higher and often this can result in a decrease in stage of prolapse especially if your prolapse is mild or has resulted from weakness and a loss of muscle. But I’m getting ahead of myself . . .
What does it look like?
A urethrocele looks like a donut around your urethra. But because everyone’s vaginal rugae looks different, it can be very difficult to know if you have a true urethrocele or what you’re seeing is the walnut or swelling or just evidence of hyper mobility.
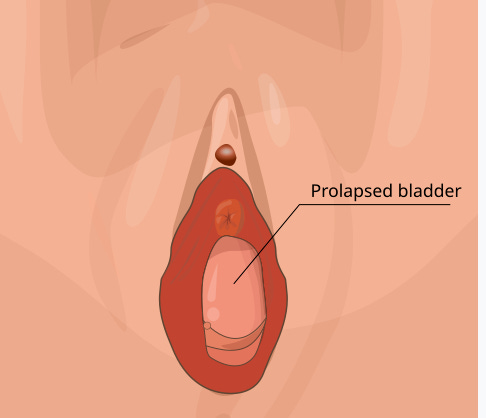
What does a cystocele look like? If you have a mild prolapse, you probably won’t see anything. If you watched the video I linked above with Dr. Fitgerald, she explains how there is no good grading system for POP. We have the POP-Q but it’s based off a moving target (the hymen) and can be skewed by the walnut. She explains how a ballooning prolapse that’s quite severe can be graded low on the POP-Q test and how a mild prolapse that hardly moves can be graded as high on the POP-Q test. So along with these numbers it’s important to ask: is there ballooning, is there a lot of movement, and would you consider this mild, moderate, or severe?
If you have a mid-level cystocele, potentially grade 2, you may be able to see the bladder at the top of the vaginal opening, or it could be hidden behind a walnut. You may also be able to feel the bulge manually. If you have 3rd or 4th degree, you may see it coming out of the opening.
In standing while bearing down if you can see a vaginal bulge, you may have prolapse, or you may just be unfamiliar with your new anatomy. That’s why it’s important to ask a trained professional. But I would caution you not to expect an OBGYN to tell you about a prolapse just because you’ve had an exam. The vast majority of women with prolapse aren’t told they have it until their doctor recommends surgery or their symptoms are so debilitating/irritating that they seek out specialized help from a Urogyn or a PFPT.
(PSST: if you’re having a prolapse test make sure you are examined in standing and laying down, relaxed and bearing down. They can even do the exam in a functional position like squatting and bearing down and even holding weight.)
The problem is everyone’s vagina looks different so this can be very difficult to discern. It’s why you need to ask a professional for a diagnosis. A rectocele looks similar to a cystocele but the bulge emerging from the back wall, so when lying down it may not be noticeable at all as gravity pulls it back. If you are working on releasing tension from your pelvic floor muscles internally or releasing your scar tissue in standing, you may feel a bulge on the back wall. Again, this could be normal.
A protruding cervix has a more distinctive look because of it’s shape, but again, it’s more useful to have a professional diagnosis.
This is the best resource available: Dr. Margo K has a support group you can request access to with real photos of what prolapse looks like, what grade it is, and how it changed over time. You have to make an account and pay for access. Once you’re in you can agree to the terms and conditions and request access to the explicit photo gallery.
What does it feel like?
I’ve heard this described so many ways: a heaviness, a dragging sensation, like a tampon is hanging out, a barrier to entry, being unable to hold in period products. None of these felt particularly right to me. For me it felt like a bubble sitting at the entrance. And during certain movements, that bubble pressed against my clothing more than at other times.
Cystocele can cause incomplete emptying of the bladder which can lead to chronic UTIs. Rectocele can cause incomplete emptying of the bowels and can mean you need to splint. This is the best resource I’ve ever seen for splinting. With either condition it is incredibly important to never bear down during voiding or defecating and to drink plenty of water and supplement with some form of laxative if you have rectocele.
Why does it happen?
Vaginal delivery (the tissues are stretched beyond their limit as the baby passes through, if forceps or vacuum used or if you had prolonged labor, prolonged pushing, or a high degree tear, you are at higher risk), subsequent pregnancy after vaginal delivery (added weight on already damaged tissue), improper lifting technique (bearing down/holding your breath), improper toileting practices (bearing down, straining, forcing out urine/stool), connective tissue disorders, genetics, and I’m sure other causes yet to be uncovered.
Who are you?
Someone who suspects prolapse but has had no children? Click HERE
A newly postpartum mom without a diagnosis? Click HERE
A postpartum mom 1+ years post delivery with or without a diagnosis? Click HERE
A PRE-menopausal woman considering or who has had surgery? Click HERE
A peri-menopausal, menopausal, or post-menopausal woman? Click HERE
If links are not highlighted, these pages are COMING SOON
*I’m making these distinctions because your hormones really matter for your recovery and what kind of treatment you might consider.
**For the sake of this newsletter I’ll be using the terms mom and woman, but please take that to be inclusive of any person with pelvic openings that can lead to pelvic descension
PSST: there are risk assessment checks than can be done before a vaginal delivery to determine how at risk you are for developing severe POP, a severe tear, or avulsion. They aren’t perfect for predicting outcomes, but knowing this can help you make an educated decision for how you would like to birth. Check out Jeanice Mitchell for what to ask for at a PT appointment to get these checks done.